Stigmas Towards Mental vs. Physical Health
Item
Poster Number
29
Poster Title
Stigmas Towards Mental vs. Physical Health
First Presenter
Brittany Pridgen
Other Contributors
Austin Taylor
Abstract
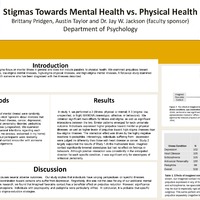
Introduction: The majority of research on mental illness stigma focus on mental illness in general and do not include parallels to physical health. We examined prejudices toward persons with low-stigma physical illnesses, low-stigma mental illnesses, high-stigma physical illnesses, and high-stigma mental illnesses. A follow-up study examined the effects of imagined positive contact with someone who has been diagnosed with the illnesses described.
Methods: In Study 1, participants (N=276, no history of mental illness) were randomly assigned to one of ten conditions in order to elicit "opinions about illnesses that can affect people and those around them": heart disease, cancer, depression, schizophrenia, HIV/Aids, psoriasis, antisocial personality disorder, pedophilia, unspecified physical illness, and mental illness (unspecified). We examined stereotypical attitudes, sentiments, and behavioral intentions regarding each illness category (e.g., unpredictable, makes me anxious, welcomed in my home). Study 2 employed a similar methodology, but participants were randomly assigned to an imagined favorable or neutral contact encounter with someone diagnosed with the illness prior to making judgements.
Results: In study 1, we performed a 2 (Illness: physical or mental) X 3 (stigma: low, unspecified, or high) MANOVA (stereotypic, affective, or behavioral). We obtained significant main effects for illness and stigma as well as significant interactions between the two. Similar patterns emerged for each univariate outcome. Individuals expressed higher prejudice toward mental vs physical illnesses, as well as higher levels of prejudice toward high-stigma illnesses than low-stigma illnesses. The interaction effect was driven by the highly negative reactions to pedophilia. Interestingly, individuals suffering from depression were judged no differently than those with heart disease or cancer. Study 2 largely supported the results of Study 1. At the multivariate level, imagined contact significantly lowered stereotypes but had no effect on feelings or behaviors. Although positive interaction was consistently in the anticipated direction for each specific condition, it was significant only for stereotypes of antisocial personality.
Discussion: The stigma associated with mental illness causes several adverse outcomes. Our study implies that individuals have varying perspectives on specific illnesses. Surprisingly, there found no indication of discrimination toward persons who suffer from depression. Regrettably, this was not the case for any of our additional mental illness conditions. Consistent with previous research, we found that imagined favorable contact has a beneficial effect on prejudice reduction. However, significance was limited to the reduction of ASPD preconceptions. Individuals with psychopathy and pedophilia were particularly vilified. In conclusion, it is probable that specific mental illnesses would necessitate specific stigma-reduction strategies.
Methods: In Study 1, participants (N=276, no history of mental illness) were randomly assigned to one of ten conditions in order to elicit "opinions about illnesses that can affect people and those around them": heart disease, cancer, depression, schizophrenia, HIV/Aids, psoriasis, antisocial personality disorder, pedophilia, unspecified physical illness, and mental illness (unspecified). We examined stereotypical attitudes, sentiments, and behavioral intentions regarding each illness category (e.g., unpredictable, makes me anxious, welcomed in my home). Study 2 employed a similar methodology, but participants were randomly assigned to an imagined favorable or neutral contact encounter with someone diagnosed with the illness prior to making judgements.
Results: In study 1, we performed a 2 (Illness: physical or mental) X 3 (stigma: low, unspecified, or high) MANOVA (stereotypic, affective, or behavioral). We obtained significant main effects for illness and stigma as well as significant interactions between the two. Similar patterns emerged for each univariate outcome. Individuals expressed higher prejudice toward mental vs physical illnesses, as well as higher levels of prejudice toward high-stigma illnesses than low-stigma illnesses. The interaction effect was driven by the highly negative reactions to pedophilia. Interestingly, individuals suffering from depression were judged no differently than those with heart disease or cancer. Study 2 largely supported the results of Study 1. At the multivariate level, imagined contact significantly lowered stereotypes but had no effect on feelings or behaviors. Although positive interaction was consistently in the anticipated direction for each specific condition, it was significant only for stereotypes of antisocial personality.
Discussion: The stigma associated with mental illness causes several adverse outcomes. Our study implies that individuals have varying perspectives on specific illnesses. Surprisingly, there found no indication of discrimination toward persons who suffer from depression. Regrettably, this was not the case for any of our additional mental illness conditions. Consistent with previous research, we found that imagined favorable contact has a beneficial effect on prejudice reduction. However, significance was limited to the reduction of ASPD preconceptions. Individuals with psychopathy and pedophilia were particularly vilified. In conclusion, it is probable that specific mental illnesses would necessitate specific stigma-reduction strategies.
Year
2022
Embargo
no embargo